Tissue repair is the body’s structured biological process of restoring damaged cells, fibers, and structures after injury, proceeding through four overlapping phases: hemostasis, inflammation, proliferation, and remodeling. Understanding how tissue repairs itself matters far beyond satisfying curiosity. It explains why some injuries heal in days while others take months, why certain wounds leave scars, and why therapies like PRP and stem cell treatment can meaningfully change outcomes. The wound healing process is not a single event. It is a coordinated sequence where platelets, immune cells, fibroblasts, and signaling molecules each play a timed, specific role. When any phase is disrupted, the entire sequence suffers.
What are the four phases of tissue repair?
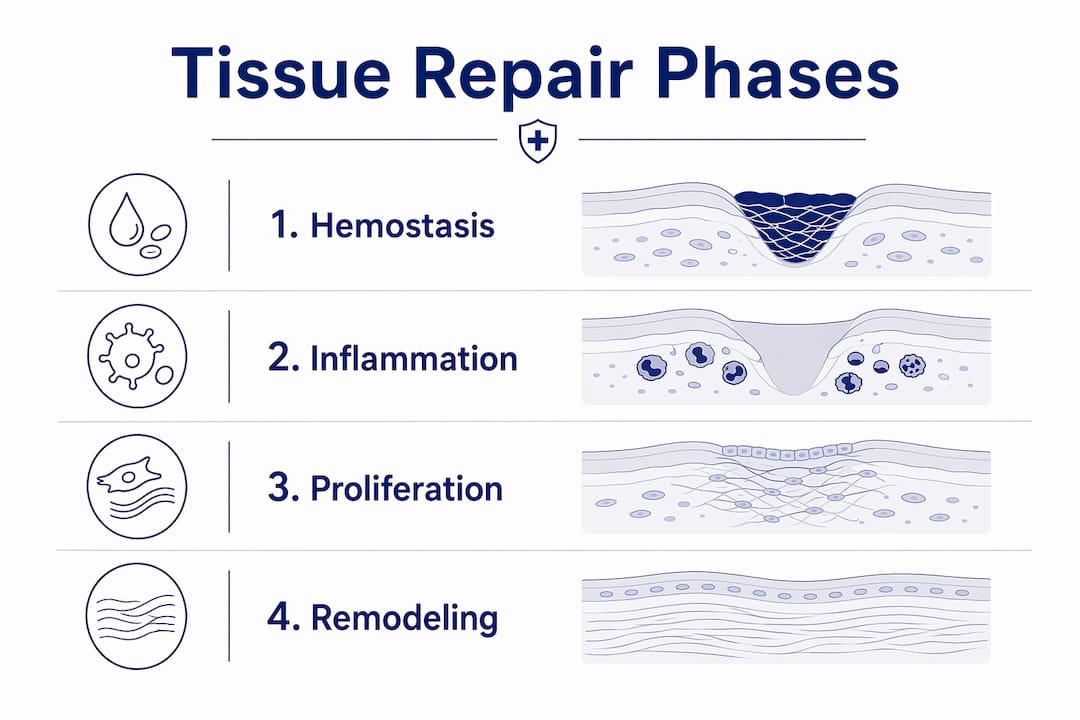
The four overlapping phases of tissue repair span from minutes after injury to a year or more, depending on wound size and tissue type. Each phase must complete properly before the next can progress, making timing and coordination critical to successful healing.
1. Hemostasis (minutes to hours)

Hemostasis is the body’s immediate response to bleeding. Platelets aggregate at the wound site and release chemical signals that trigger clot formation, sealing the injury and creating a temporary scaffold for incoming repair cells. Without this foundation, the subsequent phases cannot begin.
2. Inflammation (hours to several days)
Inflammation is not a problem to suppress. It is a necessary clearing operation. Neutrophils arrive within hours to neutralize bacteria and remove debris. Macrophages follow, consuming damaged tissue and releasing growth factors that signal the transition to active repair. Skipping or suppressing this phase prematurely, as with excessive anti-inflammatory use, can actually delay healing.
3. Proliferation (days to weeks)
Fibroblasts migrate into the wound and begin producing collagen and extracellular matrix, forming what is called granulation tissue. New blood vessels grow through a process called angiogenesis, restoring oxygen and nutrient supply. Skin cells migrate across the wound surface in a process called epithelialization, closing the wound from the edges inward.
4. Remodeling (weeks to over a year)
Remodeling is the longest and most underappreciated phase. Early collagen laid down during proliferation is primarily type III, which is weaker and less organized. Starting around three days to three weeks after injury, the body replaces type III with type I collagen, a stronger, more structured form that can last a year or more to fully mature. Scar tissue is the result of this remodeling, and it differs structurally from original tissue in both cell composition and mechanical properties.
Pro Tip: If you are recovering from a soft tissue injury, resist the urge to return to full activity the moment pain subsides. The remodeling phase is still active long after surface healing appears complete, and overloading tissue too early can disrupt collagen organization.
How do cells and signaling molecules coordinate repair?
The cellular coordination behind natural tissue healing is more precise than most people realize. Platelets are the first responders, and they do far more than stop bleeding. They release platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-β), and vascular endothelial growth factor (VEGF), all of which recruit and activate the cells needed for the next repair phases.
The immune cell sequence matters enormously. Neutrophils infiltrate wound sites within hours, followed by monocytes arriving on days two and three, differentiating into macrophages that bridge the inflammatory and proliferative phases. This transition is not passive. Macrophages actively shift their behavior from pro-inflammatory to reparative, secreting growth factors that tell fibroblasts to produce collagen and signal new blood vessel formation.
Key molecular players in this process include:
- PDGF (platelet-derived growth factor): Recruits fibroblasts and smooth muscle cells to the wound site
- TGF-β (transforming growth factor beta): Regulates collagen production and controls scar formation
- VEGF (vascular endothelial growth factor): Drives angiogenesis, the formation of new blood vessels
- IL-10 and IL-12 (interleukins): Modulate the inflammatory response, preventing it from becoming chronic
- Cytokines broadly: Act as chemical messengers that coordinate the timing and intensity of each repair phase
Research published in Nature Biomedical Engineering in 2026 found that cytokine patches accelerate healing by delivering localized IL-10, IL-12, and TGF-β to wound sites, improving repair outcomes in both rodent and porcine models. This finding confirms that the molecular signals driving repair can be externally augmented, which is the scientific basis for therapies like PRP.
Targeting immune-cell activity and cytokine signaling offers promising methods to restore normal repair processes, potentially reducing the prevalence of chronic, non-healing wounds.
How does tissue repair differ between skin and skeletal muscle?
Not all tissues heal the same way. Skin and skeletal muscle follow distinct repair pathways, and understanding the difference helps set realistic expectations for recovery.
| Feature | Skin repair | Skeletal muscle repair |
|---|---|---|
| Primary repair cells | Fibroblasts, keratinocytes | Satellite cells (muscle stem cells) |
| Stem cell involvement | Minimal | Central to the process |
| Typical outcome | Scar tissue formation | Functional muscle fiber restoration |
| Remodeling timeline | Weeks to over a year | 1 to 3 weeks for maturation |
| Key limitation | Scar tissue differs from original skin | Large defects risk fibrosis |
Skin healing follows the classic four-phase model closely. Fibroblasts produce collagen, epithelial cells migrate to close the surface, and the result is scar tissue. As noted earlier, scar tissue differs fundamentally from original skin in cell composition and mechanical properties. This is not a failure of the system. It is the body prioritizing speed of closure over perfect restoration.
Skeletal muscle operates differently. Muscle has a built-in stem cell population called satellite cells, which sit dormant alongside muscle fibers until injury activates them. Once activated, these satellite cells proliferate, differentiate into myoblasts, and fuse to form new muscle fibers. The muscle remodeling phase lasts 1 to 3 weeks for maturation, and full functional restoration also requires revascularization and reinnervation, meaning new blood vessels and nerve connections must re-establish themselves.
In skeletal muscle, macrophages play a particularly important role. They shift from a pro-inflammatory M1 phenotype to a reparative M2 phenotype, and M2 macrophages secrete growth factors that directly support fiber regeneration. When this macrophage transition is disrupted, muscle repair stalls and fibrosis, the formation of excess scar-like tissue, can replace functional muscle.
Pro Tip: For muscle injuries specifically, early controlled movement, once the acute inflammatory phase has settled, supports satellite cell activation and reduces the risk of fibrosis. Complete immobilization for extended periods can actually impair muscle regeneration.
What factors can impair or slow tissue repair?
The wound healing process is sensitive to a range of internal and external variables. Understanding what disrupts it helps explain why two people with similar injuries can have very different recovery timelines.
- Wound size and depth: Larger wounds require more collagen deposition, more angiogenesis, and longer remodeling. Deep wounds that reach muscle or bone involve multiple tissue types with different repair timelines, adding complexity.
- Blood supply and oxygenation: Oxygen is required for collagen synthesis and immune cell function. Poor circulation, common in peripheral artery disease or diabetes, significantly slows the proliferative phase and increases infection risk.
- Chronic inflammation: When the inflammatory phase does not resolve, the body cannot transition to proliferation. Chronic wounds, including many diabetic ulcers and pressure injuries, are often stuck in a persistent inflammatory state driven by dysregulated cytokine signaling.
- Impaired immune responses: Immunosuppressed patients, whether from medication, disease, or age-related immune decline, show delayed neutrophil and macrophage activity. The debris-clearing phase takes longer, and the signal for fibroblast recruitment is weaker.
- Fibrosis risk: In both skin and muscle, excessive TGF-β signaling can push repair toward fibrosis rather than functional tissue restoration. This is particularly problematic in large muscle defects, where immune and inflammatory stages must clear damage before tissue growth can begin, and any disruption to that sequence compounds the problem.
Emerging therapies, including cell-based cytokine delivery and PRP, directly target these failure points. You can read more about evidence-based healing strategies that address these specific impairments. The goal in each case is to restore the normal signaling environment so the body’s own repair sequence can proceed as intended.
Key takeaways
Tissue repairs itself through a precisely timed four-phase sequence, and disruption to any single phase, whether from poor blood supply, chronic inflammation, or premature loading, compromises the entire process.
| Point | Details |
|---|---|
| Four phases are sequential | Hemostasis, inflammation, proliferation, and remodeling must each complete before the next progresses. |
| Cells coordinate through signals | Platelets, macrophages, and fibroblasts communicate via PDGF, TGF-β, VEGF, and cytokines to drive repair. |
| Muscle and skin heal differently | Skeletal muscle relies on satellite cell activation; skin defaults to scar formation via fibroblasts. |
| Remodeling takes the longest | Collagen maturation from type III to type I can continue for a year or more after visible healing. |
| Disrupted signaling causes chronic wounds | Dysregulated cytokines and poor immune transitions are the primary drivers of non-healing wounds. |
What we see in practice, and what it means for your recovery
Felix here. After working with patients recovering from sports injuries, joint damage, and degenerative conditions, the single most consistent observation I can share is this: most people underestimate how long the remodeling phase actually takes.
Patients often come in frustrated that they still feel stiffness or reduced strength weeks after a muscle or tendon injury, even when imaging looks acceptable. What they are experiencing is a tissue that has closed but has not yet finished remodeling. The collagen is still maturing. The mechanical properties of the tissue are still changing. That is not a failure of healing. It is healing doing exactly what it should.
The second thing I want to address is the role of regenerative therapies honestly. PRP and stem cell treatments do not replace the body’s repair process. They support it by amplifying the signaling environment, particularly in cases where that environment has become dysregulated. In patients with chronic inflammation or poor blood supply, these therapies can restore the conditions the body needs to progress through its natural phases. They are most effective when used as part of a structured recovery plan, not as a standalone fix.
I also think the research on regenerative treatments in aging is worth paying attention to. As we age, satellite cell populations decline, macrophage transitions slow, and collagen quality decreases. That does not mean healing stops. It means it needs more support, and the science is catching up with practical tools to provide that.
Realistic expectations matter. Tissue repair is genuinely complex, and respecting that complexity is the first step toward a better outcome.
— Felix
How Nortex Tissue Regeneration supports your body’s healing process
At Nortex Tissue Regeneration, we work with patients whose natural repair process has stalled, whether from chronic joint pain, sports injuries, or degenerative conditions. Our PRP therapy concentrates the growth factors your platelets already produce, including PDGF, TGF-β, and VEGF, and delivers them directly to the site where repair has slowed. For patients with more significant tissue loss or muscle degeneration, our stem cell therapy supports satellite cell activation and the cellular coordination that functional regeneration requires. Both approaches are non-surgical, grounded in the same biology this article describes, and designed to work with your body’s own repair sequence rather than around it. If you are wondering whether your recovery timeline is normal or whether a targeted therapy might help, we are glad to talk through it.
FAQ
What are the four phases of the wound healing process?
The four phases are hemostasis, inflammation, proliferation, and remodeling. They overlap in timing and can span from minutes after injury to more than a year, depending on wound size and tissue type.
How long does tissue remodeling take after an injury?
Collagen remodeling begins around three days to three weeks after injury and can continue for a year or more. During this phase, weaker type III collagen is gradually replaced by stronger type I collagen as the tissue matures.
Why does skeletal muscle heal differently from skin?
Skeletal muscle relies on satellite cells, a resident stem cell population, to rebuild muscle fibers after injury. Skin primarily uses fibroblasts and defaults to scar formation, while muscle aims for functional fiber restoration through satellite cell activation, revascularization, and reinnervation.
What causes a wound to become chronic and not heal?
Chronic wounds typically result from a failure to transition out of the inflammatory phase, often driven by dysregulated cytokine signaling, poor blood supply, or impaired immune cell activity. Conditions like diabetes and peripheral artery disease are common contributors.
Can therapies like PRP actually improve how the body heals?
PRP concentrates growth factors including PDGF, TGF-β, and VEGF from your own blood and delivers them to the injury site, amplifying the signaling environment that drives natural repair. It is most effective in cases where the body’s own signaling has become insufficient or dysregulated.



